

Phalloplasty: Gender-Affirming Bottom Surgery
Medically reviewed by Ellie Zara Ley, MD on June 20, 2025.
What is a phalloplasty?
Phalloplasty is a type of gender-affirming bottom surgery that creates a penis over multiple stages of surgery using the existing genital tissue and tissue from another part of the body: often the forearm, thigh or groin. Some forms of phalloplasty can graft nerves into the phallus to allow for the possibility of heightened, erogenous sensitivity in the new penis. Here we present information about the different phalloplasty options we offer, their results, and why patients opt for them. Some of the topics we cover are phalloplasty scarring, urinating while standing, sensation, orgasms, penis size, penetrative sex (erections) and the possible stages of phalloplasty.
Your Surgical Options for Phalloplasty Explained
Types of Phalloplasty
A phalloplasty involves taking a skin flap from the body to create a phallus. At the Gender Confirmation Center (GCC), there are three donor sites we use to construct a phallus for a patient:
- The groin tissue is used in a groin flap phalloplasty
- The sensitive forearm tissue is used in a radial forearm free flap (RFF) phalloplasty
- The sensitive outer thigh tissue is used in an anterolateral thigh flap (ALT) phalloplasty
Stages of a Phalloplasty Surgery
There are multiple stages in a phalloplasty surgery. The number of stages depends on the patient’s goals, which will be determined by you and the surgeon during your consultation. Here is a brief summary of the stages we offer:
- The creation of the penis. During the first stage or stages of surgery, the skin flap is taken from the donor site, contoured into the shape of a phallus, and attached to the mons pubis. If you are undergoing an RFF or ALT procedure, the phallus is created and hangs freely after the primary operation. For a groin flap phalloplasty, there are 3 subsequent stages prior to having a free-hanging phallus.
- Urethral lengthening and scrotoplasty. In a second phase, about 6-9 months after the new penis has healed, our team can conduct a urethral lengthening (so you can urinate while standing) removal of the vagina (vaginectomy), and creation of a scrotum. Patients are also given the option of preserving their vaginal and/or natal reproductive organs. However, if a patient wishes to undergo a urethral lengthening to be able to urinate standing up, they are required to undergo a vaginectomy due to the high risk of urethral complications.
- Additional procedures: For additional stages, we can shape the tip of the phallus in a procedure called a glansplasty, insert an erectile device, testicular expanders, and testicular implants. You can read more about these additional procedures, their timeline, and recovery processes here.
Choosing Between Phalloplasty Procedures
What are the common deciding factors between the three phalloplasty types?
Patients who choose a groin flap phalloplasty often do so because:
- They are comfortable with their new phallus having a normal level of tactile sensation as opposed to heightened, erogenous sensation (exceptions are described below)
- They have a preference for the operation not leaving any sizable, visible scars (e.g., on the thigh or forearm)
- They do not mind undergoing three subsequent surgeries over the course of 6+ months to construct the new penis
- To be a candidate for a groin flap phalloplasty, patients must have a BMI no greater than 30
Patients who choose a forearm (RFF) or thigh (ALT) phalloplasty often do so because:
- They have accepted having a visible scar tissue (on their forearm or outer thigh) from a large skin graft</li
- Having a heightened, erogenous sensation in the penis is a high priority
- To be a candidate for an RFF phalloplasty, patients must have a BMI no greater than 30 and have adequate forearm anatomy to qualify for this procedure
- To be a candidate for an ALT phalloplasty, patients must have a BMI no greater than 23 and have adequate upper leg anatomy to qualify for this procedure
If you have questions about whether your anatomy qualifies you for RFF or ALT phalloplasty, you can request a free, in-person consultation with Dr. Zara Ley here.
Preparing for Phalloplasty Surgery
Candidacy Requirements
- Age: 18 or older
- Supporting documentation: Provide a support letter from a licensed gender health professional who has a well-documented and established provider-patient relationship over an extended period of at least nine months. The letter should include the following elements:
- A gender dysphoria diagnosis
- Any other existing psychiatric diagnoses and whether or not they impact the patient’s readiness for surgery
- A statement that informed consent has been obtained from the patient: that they understand the risks, benefits, and potential long-term effects of bottom surgery.
- Insurance: Please note that at this time, due to hospital restrictions, Dr. Zara Ley (she/her/they) is only able to take phalloplasty patients with insurance coverage. Providers that cover gender-affirming bottom surgery generally require that patients present a support letter and be on continuous hormone therapy for a minimum of 12 months to qualify for coverage.
- BMI: Due to health concerns around post-surgical complication risks, bottom surgery is one of the only gender-affirming procedure types in which we have BMI candidacy requirements. To qualify for a groin flap phalloplasty or RFF phalloplasty, patients must have a BMI no greater than 30. To qualify for an ALT phalloplasty, patients must have a BMI no greater than 23.
Scheduling a Surgical Consultation
The first step to any surgical journey is scheduling a consultation with a board-certified surgeon who specializes in phalloplasty. Dr. Ley (she/her/they) is the only transgender woman of color to offer a full-spectrum specialization in gender-affirming surgery: top surgery, bottom surgery, facial surgery, and body contouring.
For phalloplasty procedures, Dr. Ley requires that patients come in person to her San Francisco office to conduct an examination to verify which type of surgery the patient qualifies for. You can request a free consultation with her here.
Lifestyle Changes
Dr. Ley will not perform microsurgery (e.g., nerve reinnervation) on patients who smoke or vape, as tobacco and nicotine use significantly increase surgical risks and impair healing. If you are a current smoker, you may be required to obtain medical clearance from another healthcare provider confirming that you have been smoke-free for a designated period before surgery can be scheduled. Other positive lifestyle habits, like eating a balanced, healthy diet and exercising regularly, can help prevent surgical complications.
Hair Removal
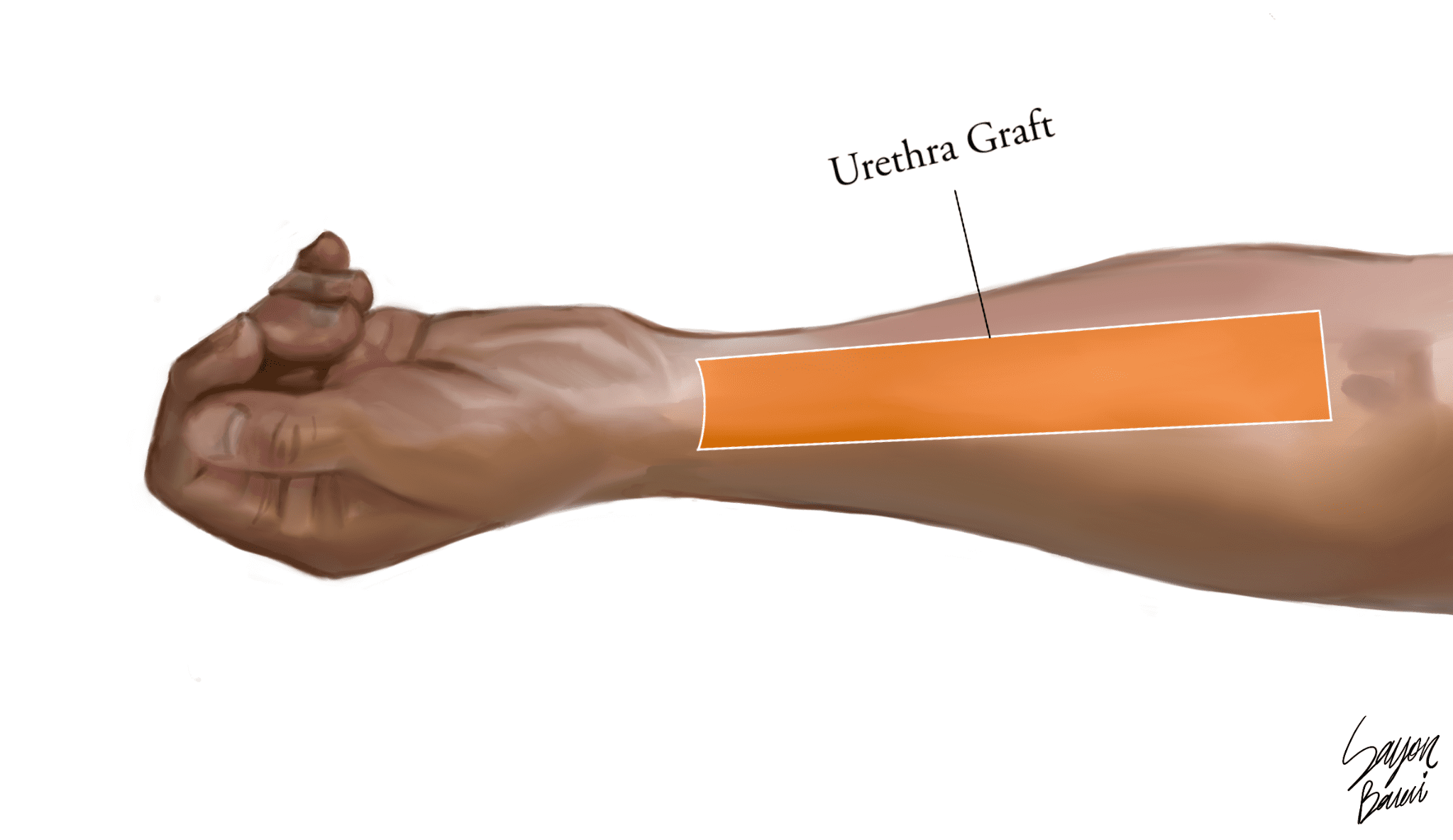
Patients who would like to undergo an RFF or ALT phalloplasty or have a urethral graft taken from the forearm or thigh must undergo electrolysis hair removal to this area prior to surgery.
Please note that permanent hair removal is only required for the section of the forearm or thigh (highlighted in orange on the illustrations) that will be used as a graft for the urethra. Complete and permanent hair removal (electrolysis) is required because hair growth inside of the urethra can cause a variety of complications. Patients may undergo hair removal of the other areas of their forearms if they wish to prevent hair growth on the phallus portion. For more information, click here.

Frequently Asked Questions about Phalloplasty Results:
How visible are phalloplasty scars?
The visibility of phalloplasty scars depends on the procedure type. Patients who get a groin flap phalloplasty will have the most concealable scars.
Patients who get a forearm (RFF) or thigh (ALT) phalloplasty will have a large rectangular swath of scar tissue visible on either their forearm or thigh. This swath of scar tissue will be depressed and discolored compared to the surrounding skin, making it look similar to a burn. It can be concealed with shorts or a long-sleeved shirt. The area can be repigmented by an experienced medical tattoo artist a year after it has healed (at least 12 months post-op).
Can a patient urinate from their penis (urinate standing up) with a phalloplasty?
During the initial construction of the phalloplasty, a urethra can be built inside of the penis to allow for a patient to eventually urinate while standing up. However, to let the phalloplasty heal, the natal urethra and the urethra in the penis are not connected until 6-9 months after the initial procedure. This means a patient will not be able to urinate out of the tip of their penis until 6-9 months later. Catheters will be used during the recovery process of each of these procedures.
What determines phalloplasty size?
The size and girth of a patient’s phalloplasty results from the unique plan you make with your surgeon during a free in-person consultation. An in-person consultation is required to determine candidacy for a phalloplasty operation. Generally speaking, the size of the patient’s body (specifically the skin flap donor site) can limit the size of the phallus.
What is the sensation like after a phalloplasty?
Nerve regeneration can start as early as three weeks after surgery, but it is different for every patient. As nerves regenerate, patients may experience tingling sensations in the site until they heal after a few months. Some patients experience no nerve regeneration at all.
Whether sensation is tactile or erogenous (heightened), it will generally be felt equally along the entire penis. The radial forearm flap (RFF) and anterolateral thigh flap (ALT) phalloplasty can give patients a heightened, erogenous sensation in their penis since the nerves used in the donor site (the forearm or the outer thigh) allow for more sensation.
The groin flap phalloplasty allows for tactile sensation as opposed to erogenous sensation. That said, if a patient opts for a urethral lengthening using a smaller skin graft from the forearm, erogenous sensation can be established through nerve innervation microsurgery.
Is orgasm possible after phalloplasty?
If your phalloplasty involves preserving erogenous sensation, orgasms are possible through stimulating the penis. Patients should wait 3-4 months (or until incisions are fully healed with approval from your surgeon) before masturbating or engaging in other kinds of sexual activity with the new penis. With a completed urethral lengthening, some patients report being able to ejaculate clear fluid when they orgasm.
How soon can a patient have penetrative sex after a phalloplasty?
3-4 months after an RFF or ALT phalloplasty is constructed (or when incisions have fully healed), a patient can begin engaging in sexual activity with their new penis, alone or with partners. For a groin flap phalloplasty, this is about 6+ months after the first surgery.
Can a patient experience erections with a phalloplasty?
To have penetrative sex with a phalloplasty, a patient can use the assistance of a silicone erectile sleeve and/or a penis pump after they have fully healed and have received clearance from their surgeon. 12 months after the phalloplasty is constructed, a patient can have an erectile device inserted: a malleable rod or a saline pump system. You can read more about these options here.
Groin Flap Phalloplasty
- Groin flap phalloplasty uses groin tissue to create the new penis. Using groin tissue allows the scars from this surgery to be easily concealed, and allows a penis of adequate length and girth for most patients.
- The groin flap does not have erogenous sensation; most patients experience normal levels of tactile sensation in their new penis.
If a patient wishes to urinate standing up, our surgeon can perform a urethral lengthening using a forearm flap.- An advantage of a radial forearm flap for radial forearm urethral lengthening is that nerve innervation microsurgery can be performed. This allows for the possibility of erogenous sensation to be felt in the new penis, as a sensory nerve is also taken from the forearm and connected to a clitoral nerve. Second, the skin graft that is taken from the forearm is relatively small compared to a radial forearm free flap phalloplasty (typically 2 inches by 7 inches) and will later be covered up by a full-thickness skin graft. This procedure carries its own unique set of risks and complications.
- A groin flap can be easily concealed since it is usually covered by clothing. That said, it does not allow for the possibility of heightened, erogenous sensation to be felt in the penis unless a patient chooses to add a urethra later on through a radial forearm urethral lengthening.
- A groin flap phalloplasty procedure requires three subsequent surgeries over the course of 6+ months to create the new penis.
- The first stage involves the creation of the new penis in the form of a “suitcase” handle, for about 2+ months. Patients can expect to spend two nights in the hospital after their first stage of groin flap phalloplasty. Through the next two stages, the penis is slowly detached and left to hang freely. The “suitcase” handle stage allows the penis to maintain its blood flow to be dependent on its blood supply.
- During the third and final release, the “suitcase” handle flap is fully released, allowing the penis to detach from the groin and remain connected only at its base.
- If a patient would like to urinate out of the tip of their penis, a urethral lengthening can be conducted during a later stage.
RFF Phalloplasty and ALT Phalloplasty
- The RFF phalloplasty takes a large skin graft from the sensitive forearm region to construct a phallus. The ALT phalloplasty takes a large skin graft from the sensitive anterolateral thigh region to construct a phallus.
- Nerve innervation microsurgery allows the patient to experience erogenous sensation in their penis by hooking up one of the clitoral nerves to the sensory nerve of the forearm or thigh. A very noticeable scar is left on the forearm or thigh from the skin graft. 2-4 weeks after the flap is taken from the forearm, Dr. Ley will cover the donor site with a split or full-thickness skin graft from the thigh.
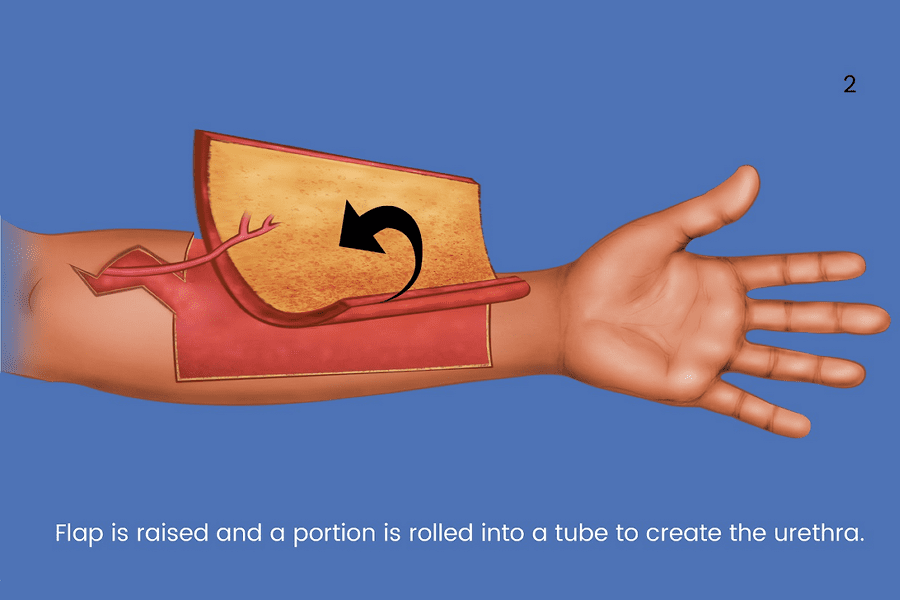
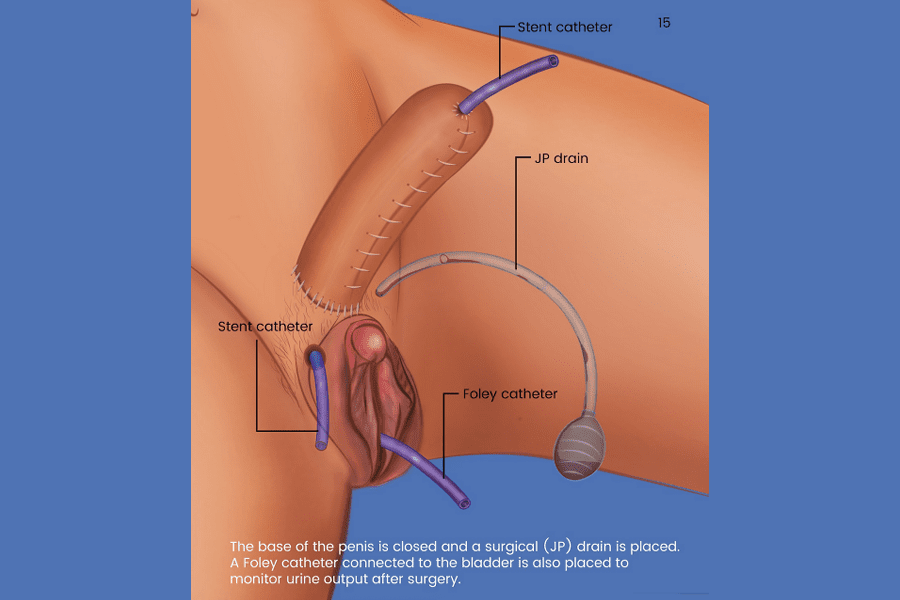
- The illustrations below demonstrate what steps are involved in an RFF phalloplasty, which is similar to the ALT. Specifically, we show the construction of a penis, the lengthening of the urethra and how the nerves are “hooked up” to allow for erogenous sensation.
Step by Step: Radial Forearm Flap (RFF) Phalloplasty
The following medical illustrations represent the construction of the new penis in an RFF phalloplasty:













Phalloplasty vs. Metoidioplasty
Metoidioplasty is a much simpler procedure than a phalloplasty. It requires fewer surgeries, has faster recovery times, and minimal scarring.
Due to different BMI requirements, some patients who are interested in getting a phalloplasty first undergo a metoidioplasty while they lose weight.
To read more about how patients make the decision between these two bottom surgery procedures, click here.
Recovery and Healing
- Hospital stay: After a microsurgical RFF or ALT phalloplasty, patients can expect to stay in the hospital for six nights. After the first stage of a groin flap phalloplasty, patients can expect to stay 2 nights in the hospital. This is when the most amount of pain, inflammation, and bruising will occur.
- Urinary catheter: A urinary catheter will be required for bottom surgery that involves the urethra. The catheter will stay in place for 2-3 weeks to drain any urine from the bladder to allow the lengthened urethra to heal. While an indwelling catheter is not painful, it may be unusual for patients to adjust to. Bladder spasms may be experienced and can be a source of discomfort that can be managed with certain medications.
- Sexual activity: We ask patients who undergo phalloplasty to completely avoid manual or oral stimulation for at least 3-4 months (or longer, depending on your healing). Your phallus is still healing and at a higher risk of infection. Patients should get their surgeon’s approval after 3-4 months before engaging in manual or oral stimulation of the phallus.
For more detailed instructions about phalloplasty recovery, click here.
Click Here to Request the Next Steps to Schedule a Consult!
We offer complimentary virtual and in-person consultations with our board-certified surgeons. Click here to complete our consultation request form to learn more about the next steps in your patient journey.
BOOK CONSULTATION
Suite 1010, 450 Sutter St
San Francisco, CA 94108
Phone: (415) 780-1515
Fax: (628) 867-6510
GCC business hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
Board Certification
& Memberships
Copyright © 2023 GCC (Gender Confirmation Center). All Rights Reserved.