


How is Bottom Surgery Done?
Medically reviewed by Jennifer Richman on Dec 8, 2025.
Bottom surgery refers to a series of genital reconstruction procedures that help treat a patient’s gender dysphoria and experience greater alignment between their gender and their body. Feminizing or “MTF” bottom surgery procedures include orchiectomy (testicle removal), vulvoplasty (“zero-depth vaginoplasty”) and vaginoplasty. Masculinizing or “FTM” bottom surgery procedures include hysterectomy (removal of the uterus), vaginectomy (removal of the vaginal canal), metoidioplasty and phalloplasty.
Qualified transgender and non-binary patients can choose from the aforementioned procedure. Please note that many types of bottom surgery require multiple stages of surgery to give a patient their final desired result. You can request a free bottom surgery consultation to make a unique surgical plan tailored to your goals and anatomy.
Interested patients can review the following steps for how to undergo transfeminine bottom surgery:
Age and Informed Consent
Patients must be at least 18 years old and mentally capable of participating in an informed consent process to undergo bottom surgery.
Requesting a Consultation
The first step in anyone’s surgical journey is scheduling a consultation with a board-certified surgeon. Dr. Zara Ley (she/they) currently offers free consultations for bottom surgery, top surgery, body contouring and facial surgery; you can request one with her here. Please note that for some bottom surgery procedures, Dr. Ley requires patients come in-person to her San Francisco office to complete a physical examination.
BMI Limitations
For some types of bottom surgery, there are BMI qualification cutoffs. For a vaginoplasty, patients must have a BMI of 34 or less. Vulvaplasty patients must have a BMI no greater than 38.
Health Requirements
In order to undergo bottom surgery, patients should be in good overall physical health. Patients must quit tobacco and nicotine consumption 3-4 weeks prior to surgery or, ideally, earlier.
Support Letter
Patients who are undergoing bottom surgery for the first time must present two support letters from gender-affirming care providers that have a long-standing relationship with the patient (at least 9 months of providing service). One of these letters should be from a licensed mental health professional, whereas the other can be from a patients’ hormone therapy provider.
Please note that if you would like your insurance provider to cover bottom surgery, you may have to meet their specific requirements. For example, some insurance providers require that at least one of the support letters for bottom surgery come from a licensed mental health provider with a doctorate degree (e.g., PhD, PsyD, etc.). You can confirm these requirements with your insurance provider or by calling our office: (415) 780-1515
Hair Removal
Patients interested in undergoing a vaginoplasty or vulvaplasty will need to undergo permanent hair removal on the scrotum and/or penile shaft.
Vaginoplasty: A Step-by-Step Guide
At this time, Dr. Ley (she/her/they) only offers a two-stage penile-inversion vaginoplasty procedure for her patients. The penile-inverson technique has the most long-term evidence to support its durability and long-term patient satisfaction.
Likewise, Dr. Ley conducts vaginoplasty and vulvoplasty in two stages because patients tend to be much more satisfied with their results. In the first surgery, Dr. Ley will construct the clitoris, vulva and vaginal canal. In the second labiaplasty procedure, she will add more defined aesthetic details, such as clitoral hooding, full labia minora, and alterations the overall configuration of the labia majora. This allows her to correct any functional issues, asymmetry or aesthetic concerns a patient may have.
The following is a step-by-step guide to how a vaginoplasty is conducted.
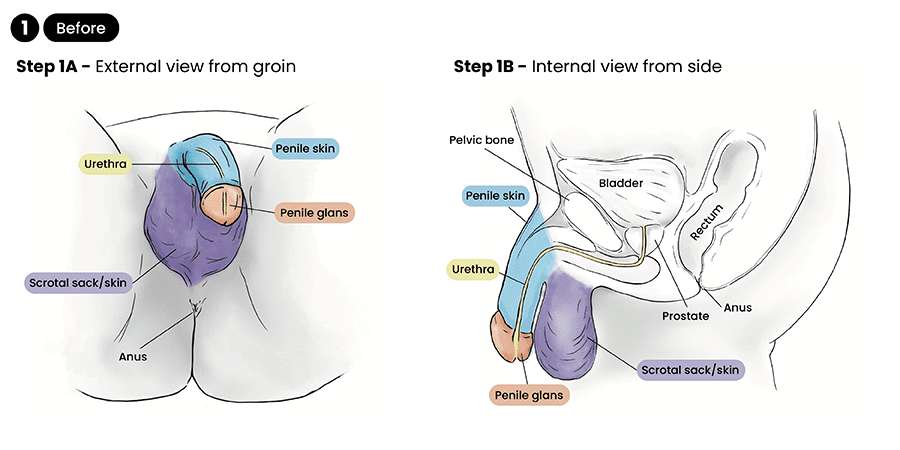
Step 1: Before
Please note that amongst the qualifications for this surgery, vaginoplasty patients must have a BMI of 34 or less. Vulvaplasty patients must have a BMI no greater than 38. Likewise, patients may need to undergo permanent hair removal of the penile shaft and scrotum prior to surgery.
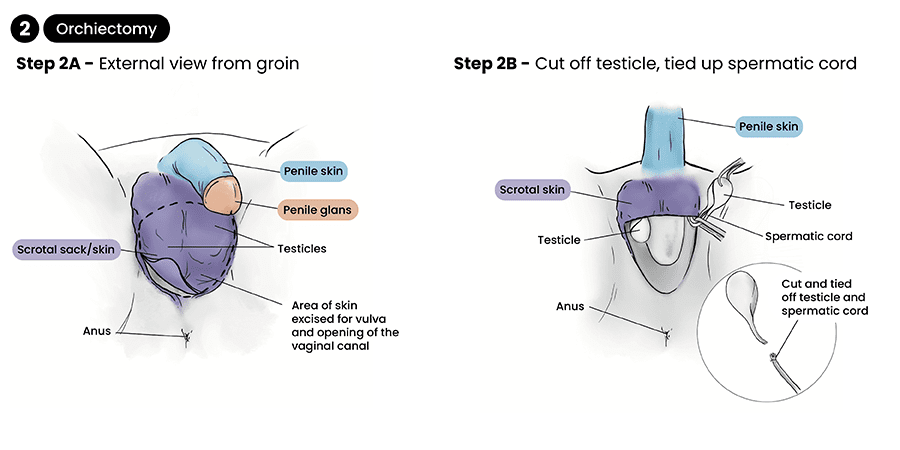
Step 2: Orchiectomy
Patients can undergo an orchiectomy (testicle removal) 8-12 weeks prior to surgery or it can be conducted at the same time as a vaginoplasty. If patients undergo an orchiectomy before vaginoplasty, their scrotal skin should be preserved so it can be used in the construction of the labia and the vaginal canal. Testicles will be sent for pathology testing after removal.
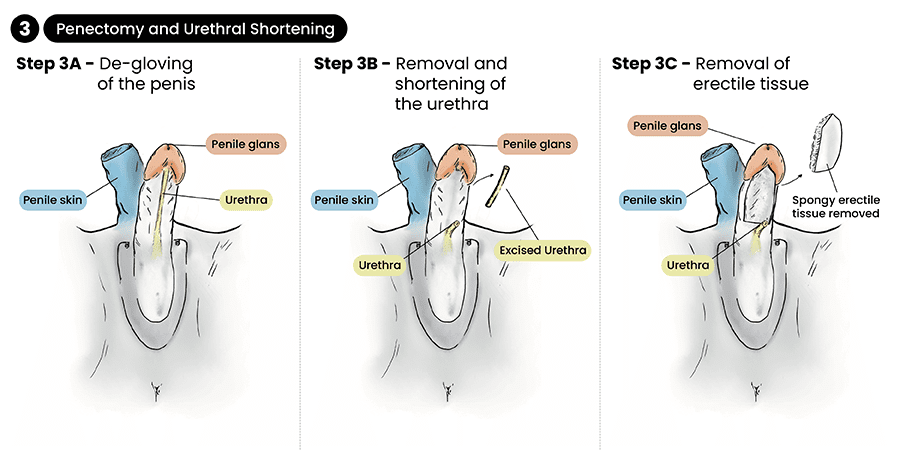
Step 3: Penectomy and Urethral Shortening
In this stage of surgery, the penis is de-gloved, meaning that the skin is separated from the shaft so that it can be used for the lining of the vaginal canal. The erectile tissue is then removed from the penis shaft and the urethra shortened.
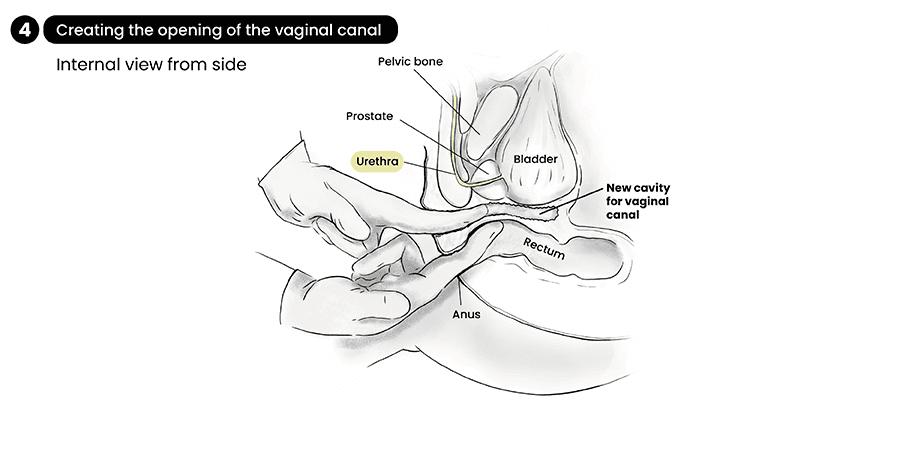
Step 4: Creating the Opening of the Vaginal Canal
A cavity is created so that the vaginal canal is positioned below the prostate and above the rectum. Depending on a patient’s anatomy, the vaginal canal typically has a depth of 5-6”.
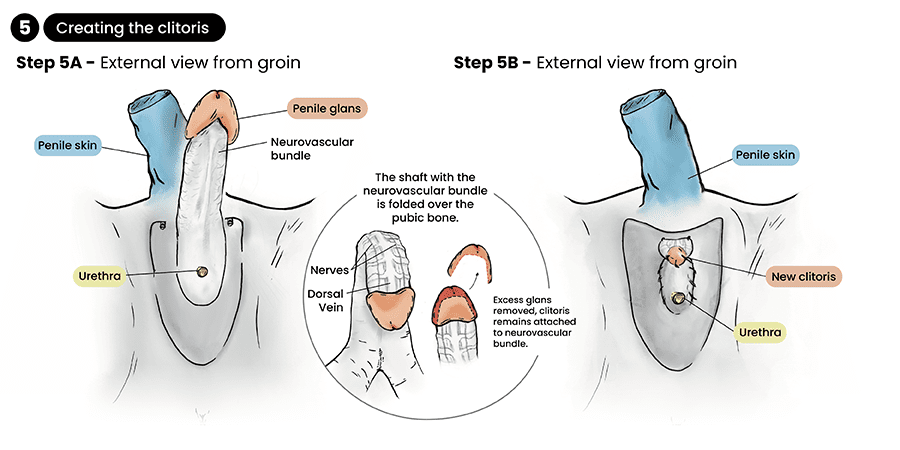
Step 5: Creating the Clitoris
After the penis is removed, the glans will still be connected to their original blood and nerve supply. The penile glans is re-sized and positioned at the top of the vulva, becoming the clitoris.
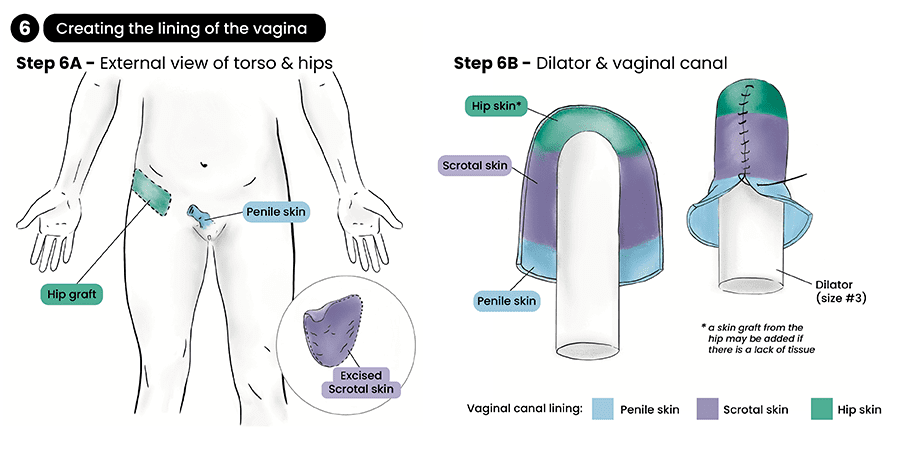
Step 6: Creating the Lining of the Vaginal Canal
In this stage of surgery, Dr. Ley constructs the lining of the vaginal canal. Grafts will be taken from the penile skin and the scrotal skin. If more tissue is needed, a skin graft from the hip can be added, leaving a scar at the top of the leg or around the groin.
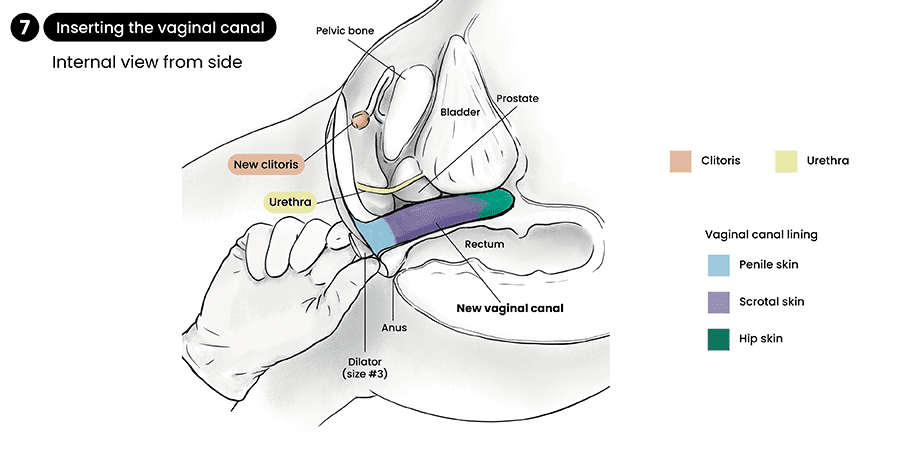
Step 7: Inserting the Vaginal Canal
Once the vaginal lining has been constructed and placed around a dilator, the dilator is placed inside of the patient’s new vaginal cavity. The vaginal canal will then be lined with packing.
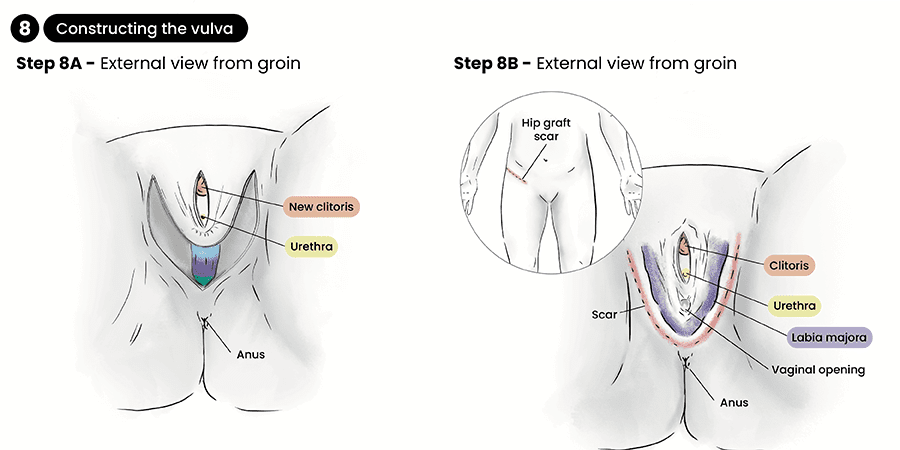
Step 8: Constructing the vulva
The final step of surgery is creating the vulva. With Dr. Ley’s two-stage technique, a patient will finish the first stage of surgery with a fully-functional clitoris, vagina, urethra and labia. In the second labiaplasty procedure, the labia minora and clitorial hood will be constructed, and any other functional or aesthetic concerns resolved.
Phalloplasty: A Step-By-Step Guide
There are multiple types of phalloplasty that Dr. Ley performs: groin flap, anterolateral thigh (ALT) flap and radial forearm flap (RFF) phalloplasty. These procedures construct a penis using skin and other tissues from another part of the body. If you are interested in seeing which type of phalloplasty you qualify for, and which procedure types can best help you meet your goals, you can request a free consultation here.
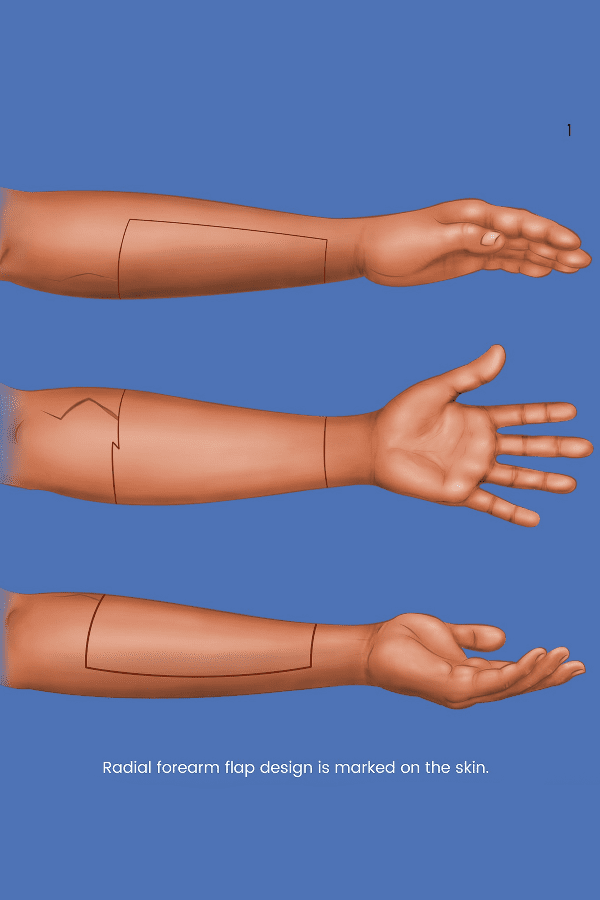
The illustrations below show how an RFF phalloplasty is conducted:
Step 1: Before
Prior to surgery, patients will need to undergo permanent hair removal of the areas of the forearm that will be used in surgery. Likewise, since the RFF procedure involves nerve innervation microsurgery––taking the sensitive nerves from the forearm and grafting them to the clitoris to give the penis heightened sensation––patients who consume tobacco and nicotine do not qualify for this surgery.
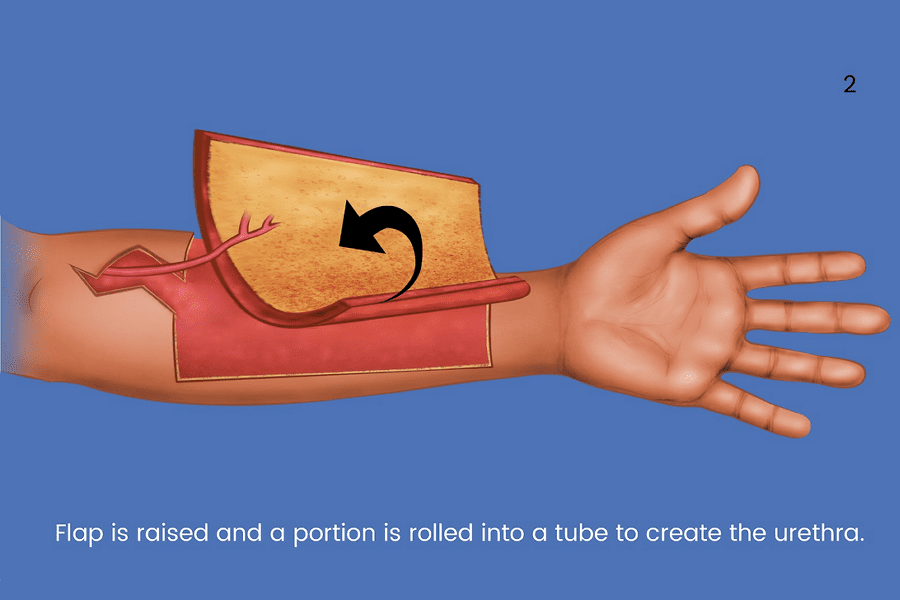
Step 2: Taking the Radial Forearm Flap & Creating the Urethra
In this stage of surgery, a flap of skin, called a full-thickness skin graft, is removed from the forearm. A portion of the flap is rolled up to create the urethra. This will go inside of the penis shaft to extend the existing urethra so that urine exits at the tip of the penis.
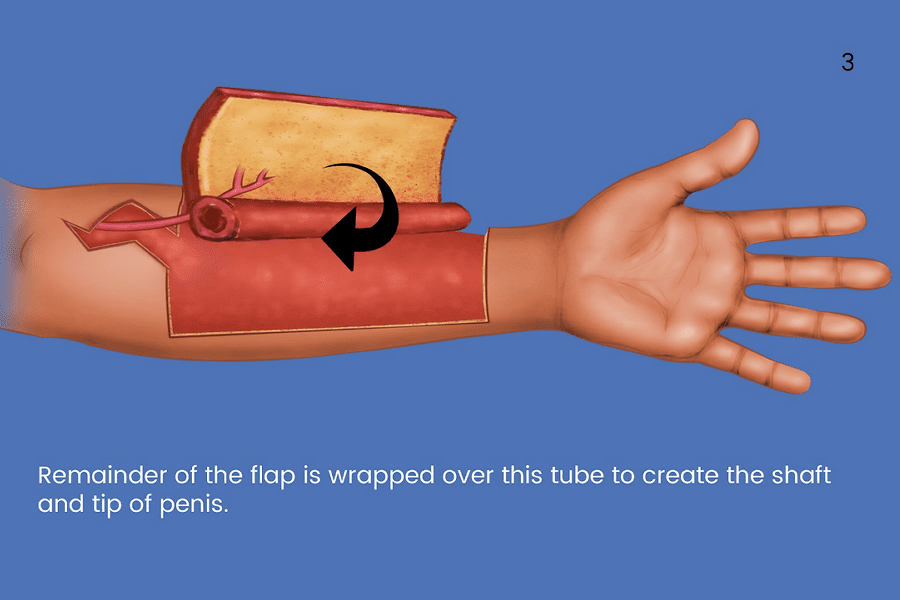
Step 3: Creating the Penis Shaft
The rest of the full-thickness skin graft from the forearm is rolled up into a tube to create the penis shaft and tip.
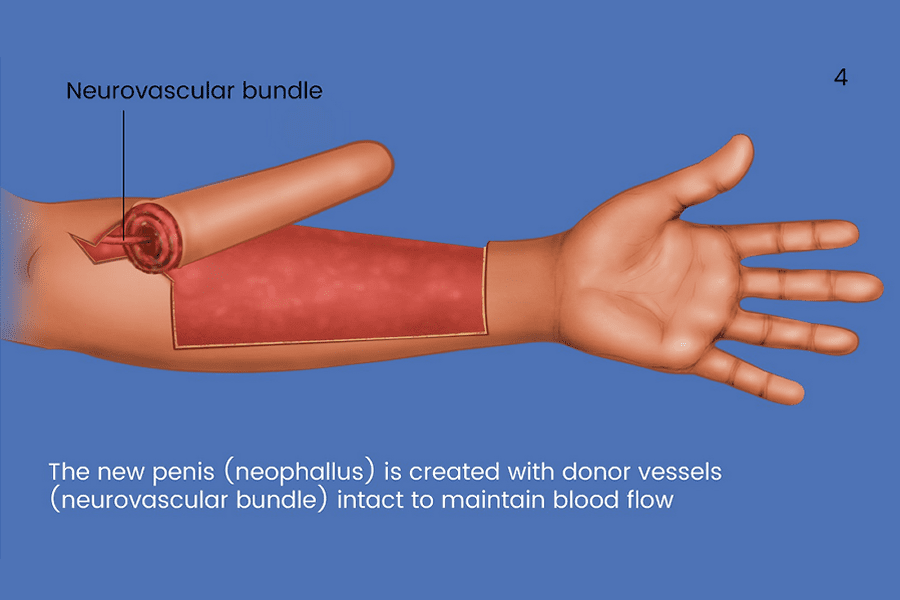
Step 4: Taking the Neurovascular Bundle from the Forearm
The forearm’s radial artery and nerves are taken and attached to the penis, giving it a blood and nerve supply.
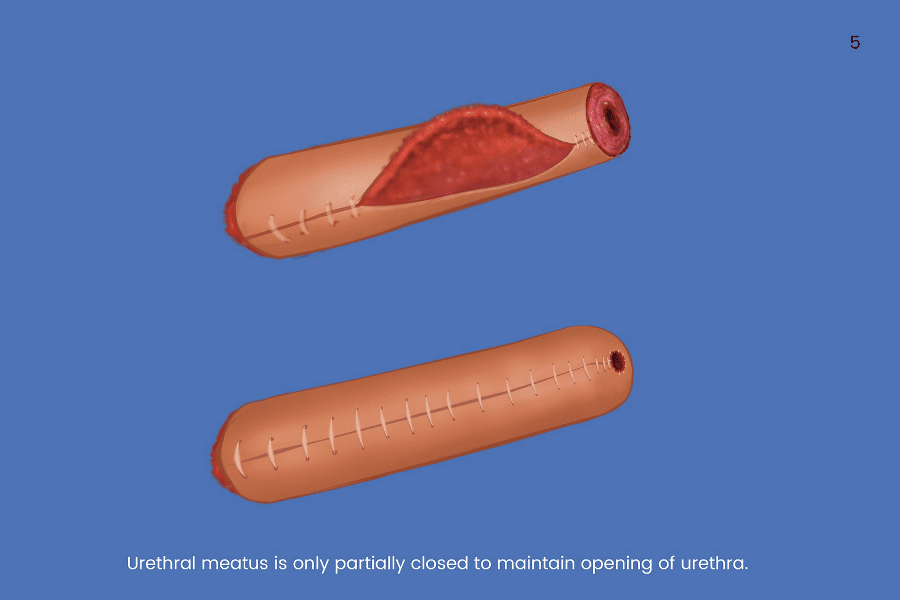
Step 5: Closing up the Phallus
Here, the phallus skin graft is closed, with a small opening left at the tip for the urethral exit.
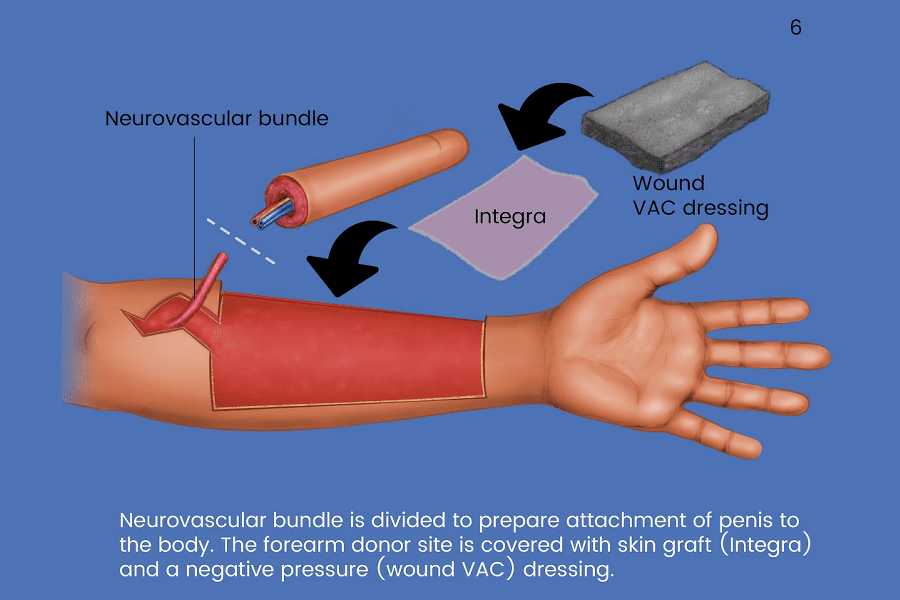
Step 6: Finishing the Forearm Graft
The neurovascular bundle is detached from the forearm so that it is connected to the penis. Then, a split-thickness skin graft (usually taken from the thigh) is placed over the open wound on the forearm, alongside a negative pressure wound dressing.
Step 7: Checking Bloodflow in the Forearm
Once the open wound on the forearm is dressed and closed, your surgeon will put it in a splint.

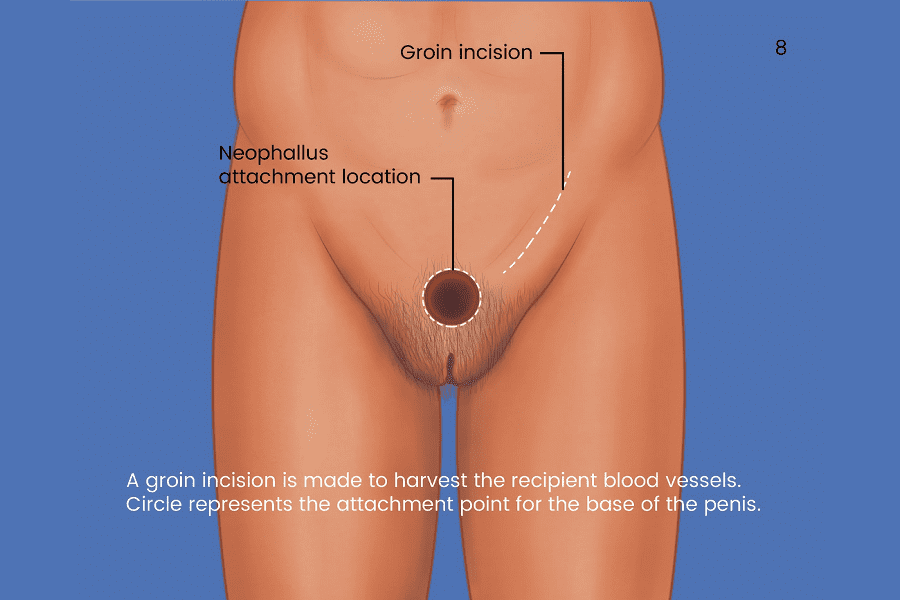
Step 8: Creating the Phallus Attachment Location
The phallus will be attached on the groin, indicated by the circle. Another incision is made on the groin to access blood vessels.
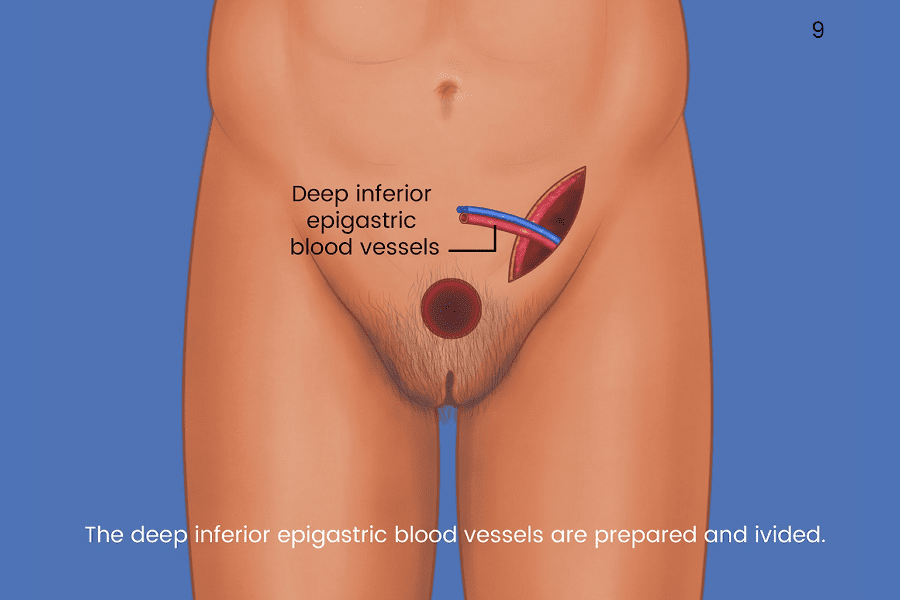
Step 9: Preparing the Blood Vessels
From the groin incision, blood vessels are drawn out that will be used to give the phallus a blood supply.
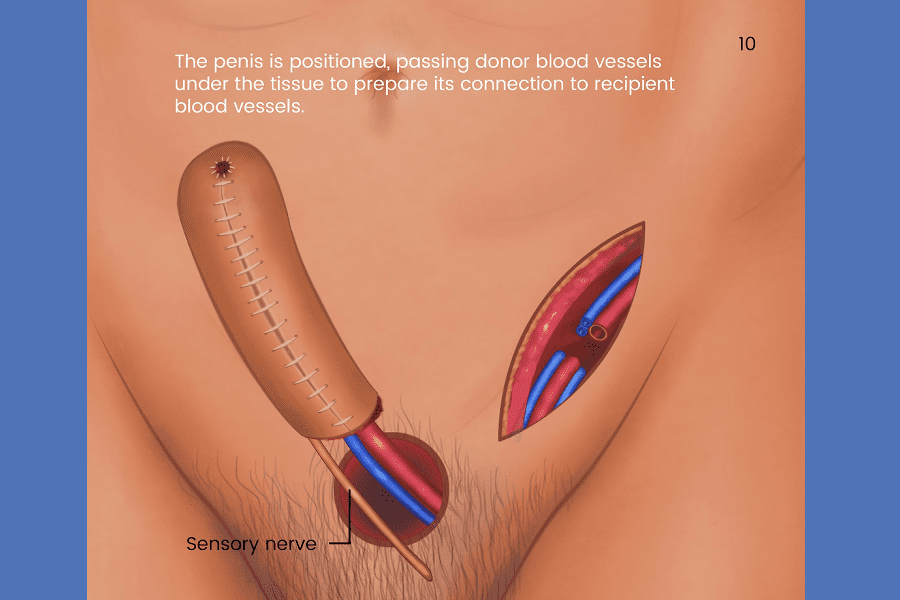
Step 10: Connecting the Blood Vessels
The donor blood vessels in the phallus (from the forearm) are connected to the veins and arteries in the groin.
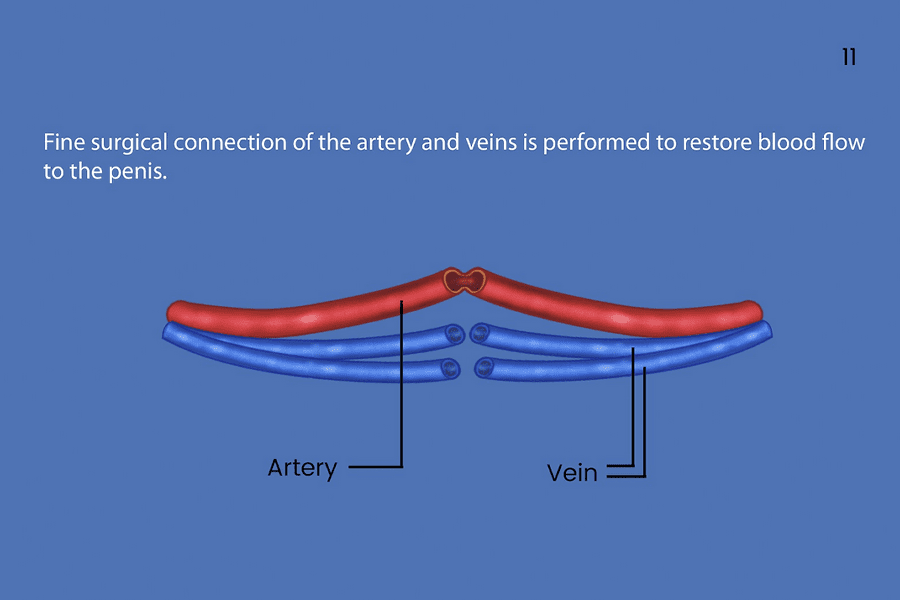
Step 11: Microsurgery to Connect Blood Vessels
Dr. Ley will perform microsurgery to attach the blood vessels from the phallus to the blood vessels in the groin. This is to provide the penis with blood supply.
Step 12: Stent Catheter Placement
A stent catheter is placed in the phallus, exiting out of the tip.
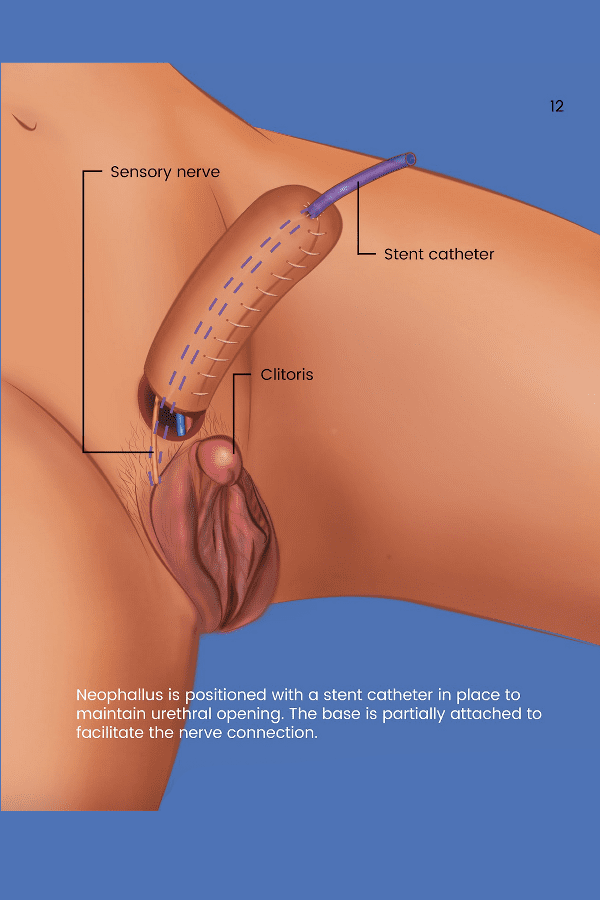
Step 13: Catheter and Nerve Placement
The stent catheter will exit around the top of the labia majora. The nerve in the penis (from the forearm) is drawn out.
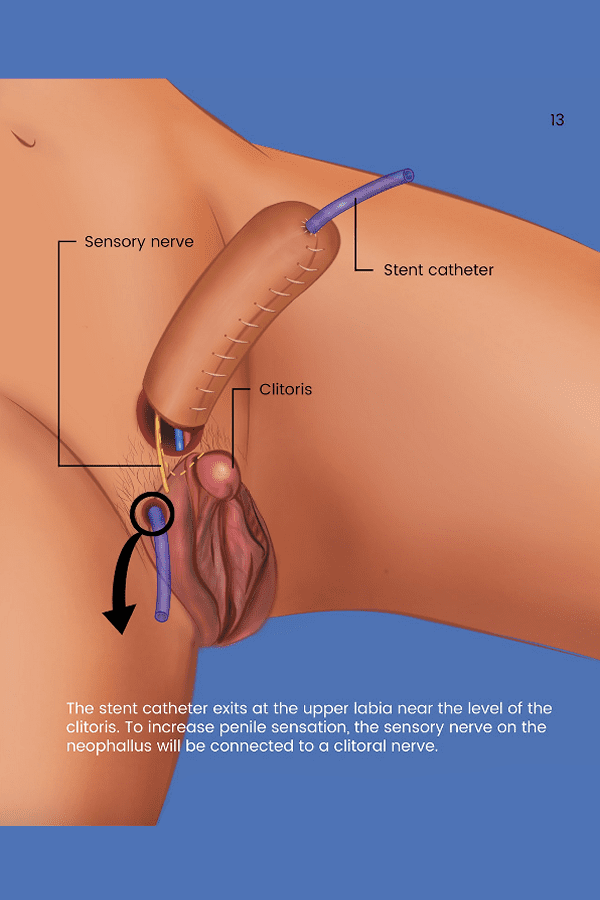
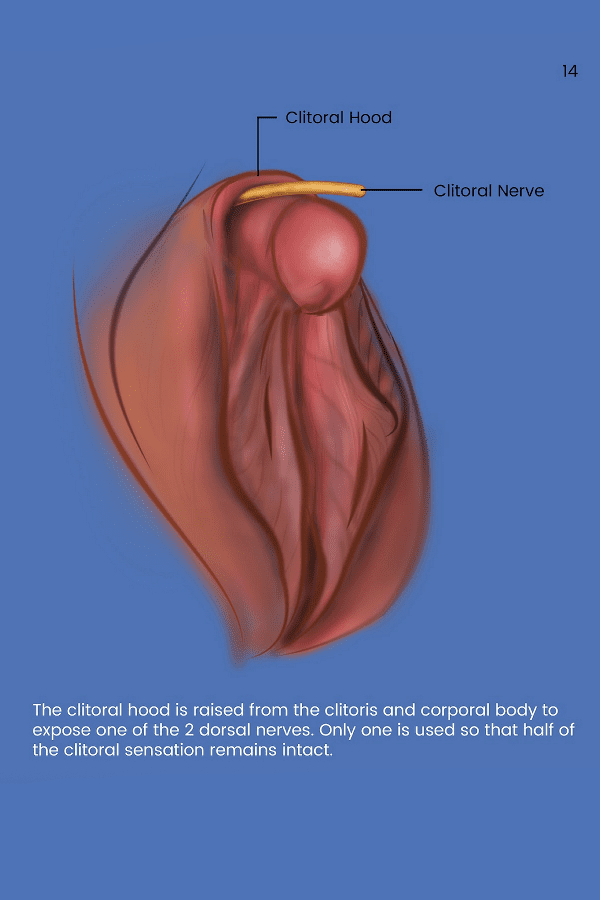
Step 14: Nerve Grafting from the Clitoris
The dorsal nerves of the clitoris are exposed. Dr. Ley will take one of the two and connect it to the nerve in the penis (from the forearm) through microsurgery. The second dorsal nerve will remain connected to the clitoris.
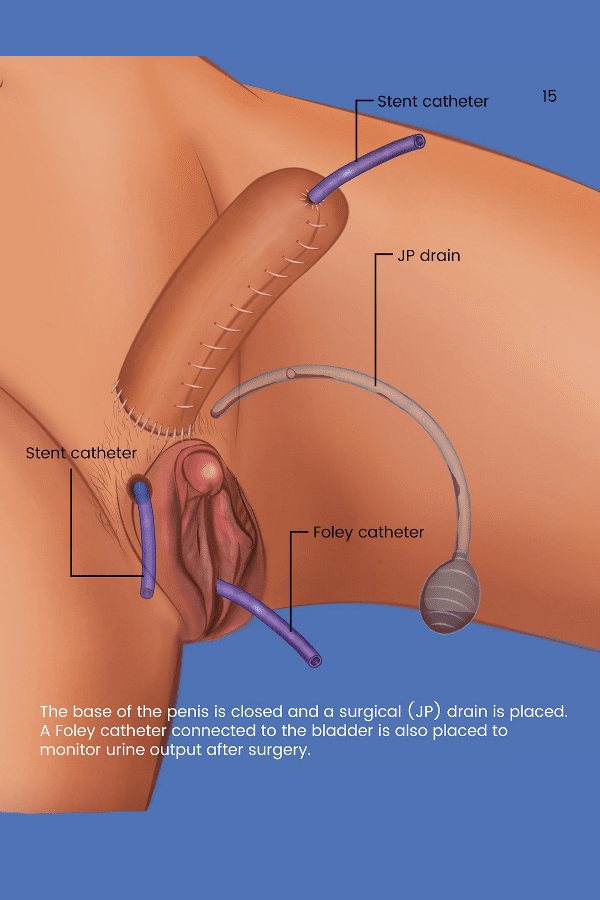
Step 15: Placing the Drain and Foley Catheder
A foley catheter is placed at the site of the original urethral opening, connecting it to the bladder, alongside a surgical drain.
 Facebook
Facebook