

The Definitive Guide to FTM Bottom Surgery

Medically reviewed by Jennifer Richman on July 2, 2025.
What is FTM Bottom Surgery?
Female-to-male (FTM) bottom surgery refers to procedures that alter the external and internal reproductive organs. “Masculinizing” bottom surgery procedures for trans and non-binary individuals include metoidioplasty, phalloplasty, and others such as vaginectomy, mons resection, scrotoplasty, hysterectomy, and more.
While the term “FTM” is generally considered to be outdated, we use it out of recognition that trans men and transmasculine non-binary folks search for this term for information on surgical transition.
Regardless of your identity, if you are interested in any of the bottom surgery procedures listed below, you can request a free, in-person consultation with Dr. Ley (she/her/they) today.
Frequently Asked Questions (FAQ)
Will I be able to achieve erections and experience sexual pleasure after FTM bottom surgery?
While the ability to achieve erections and experience sexual pleasure can vary from individual to individual, many patients report positive outcomes in terms of sexual function and satisfaction after metoidioplasty or phalloplasty. For metoidioplasty patients, the new phallus can maintain its ability for erections and sexual stimulation as the natal erectile tissue is preserved.
For phalloplasty patients, nerve innervation surgery (e.g., in an RFF phalloplasty) connects the penis to the clitoral nerve, giving it the possibility of heightened sensation. Phalloplasty patients can use silicone erectile sleeves or have an erectile device surgically implanted into their phallus to facilitate penetrative sex.
How long is the recovery period after FTM bottom surgery?
The recovery period after masculinizing bottom surgery can be extensive, especially if you undergo multiple stages of surgery. The specific timeline depends on the type of surgery performed (metoidioplasty or phalloplasty).
Will I be able to urinate standing up after FTM bottom surgery?
For both metoidioplasty and phalloplasty patients, the ability to urinate standing up is achieved through primary urethral lengthening (PUL) or reconstruction. By extending the urethra so it ends at the tip of the penis, patients are able to more easily urinate while standing, experience greater gender euphoria, and often feel safer using the men’s restroom. To prevent urinary complications, if you request to undergo a PUL with the GCC, you will need to undergo a simultaneous vaginectomy or removal of the vaginal canal.
What if I have to travel for surgery or have few people to care for me during recovery?
Having a strong support network is essential when recovering from bottom surgery. Patients will likely need help with household chores, preparing meals, bathing themselves and more. The amount of time patients spend bed-bound, in pain and dealing with inflammation can be very emotionally taxing.
For those who are traveling into the San Francisco Bay Area, we recommend that you consult our free travel guide for tips on saving money and finding trans-friendly resources, like the Quest House recovery center for transmasculine bottom surgery patients.
Types of FTM Bottom Surgery
What is commonly referred to as masculinizing or “FTM” bottom surgery can be categorized into two types. Extirpative procedures involve the removal of reproductive organs (i.e., hysterectomy, oophorectomy, vaginectomy). Reconstructive procedures (i.e., metoidioplasty, phalloplasty) have functional and aesthetic purposes: they can enlarge the penis and/or help with functions like standing to urinate or facilitate penetrative sex.
There is no prescribed surgical path that trans and non-binary patients must follow to live as their gender. Rather, patients choose which procedures to undergo based on their unique needs (such as reducing gender dysphoria), embodiment goals, and whether or not they meet the candidacy requirements.
Removal of Reproductive Organs
Hysterectomy and Oophorectomy
If you are thinking about an oophorectomy, you can learn more about bone health in trans individuals here.
Vaginectomy
Genital Reconstruction Surgeries
If you are interested in a metoidioplasty, phalloplasty, or a revision procedure, you can request a free, in-person consultation with Dr. Ley (she/her/they) today. If you would like to learn more about the deciding factors between metoidioplasty and phalloplasty procedures, click here.
Metoidioplasty


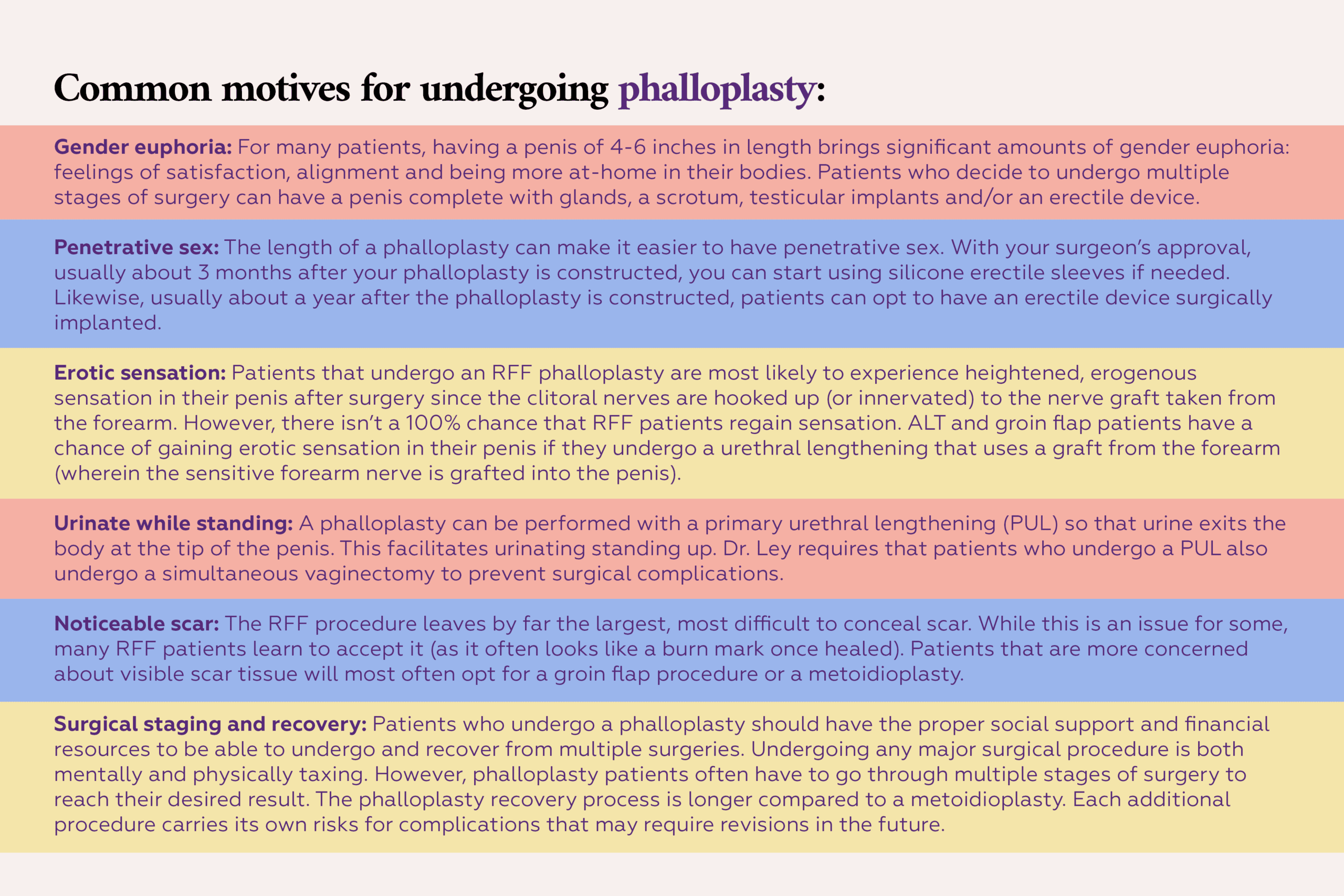
Phalloplasty
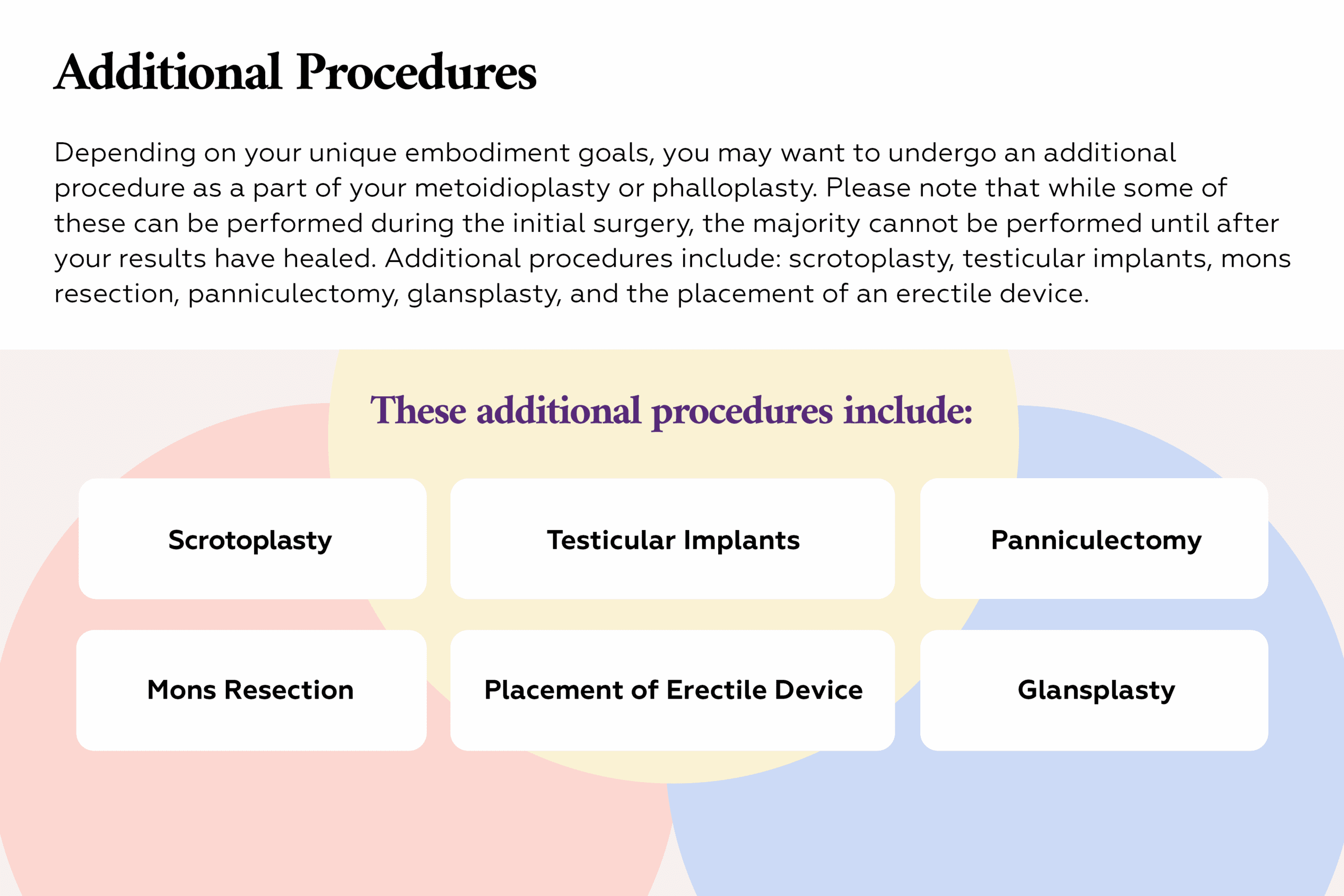
Additional Procedures
Preparing for FTM Bottom Surgery
Preparing for FTM bottom surgery is a multifaceted process that requires careful consideration and planning. Here are some key steps:
- Fertility Preservation: Consult with reproductive/fertility specialists to consider fertility preservation options.
- Surgical Consultations: For bottom surgery procedures, consultations must be in-person to determine surgical candidacy and make a surgical plan. Dr. Ley (she/her/they) is a former patient and one of the only trans surgeons of color who offers these procedures. You can request a free consultation with her to have any of your questions about bottom surgery answered.
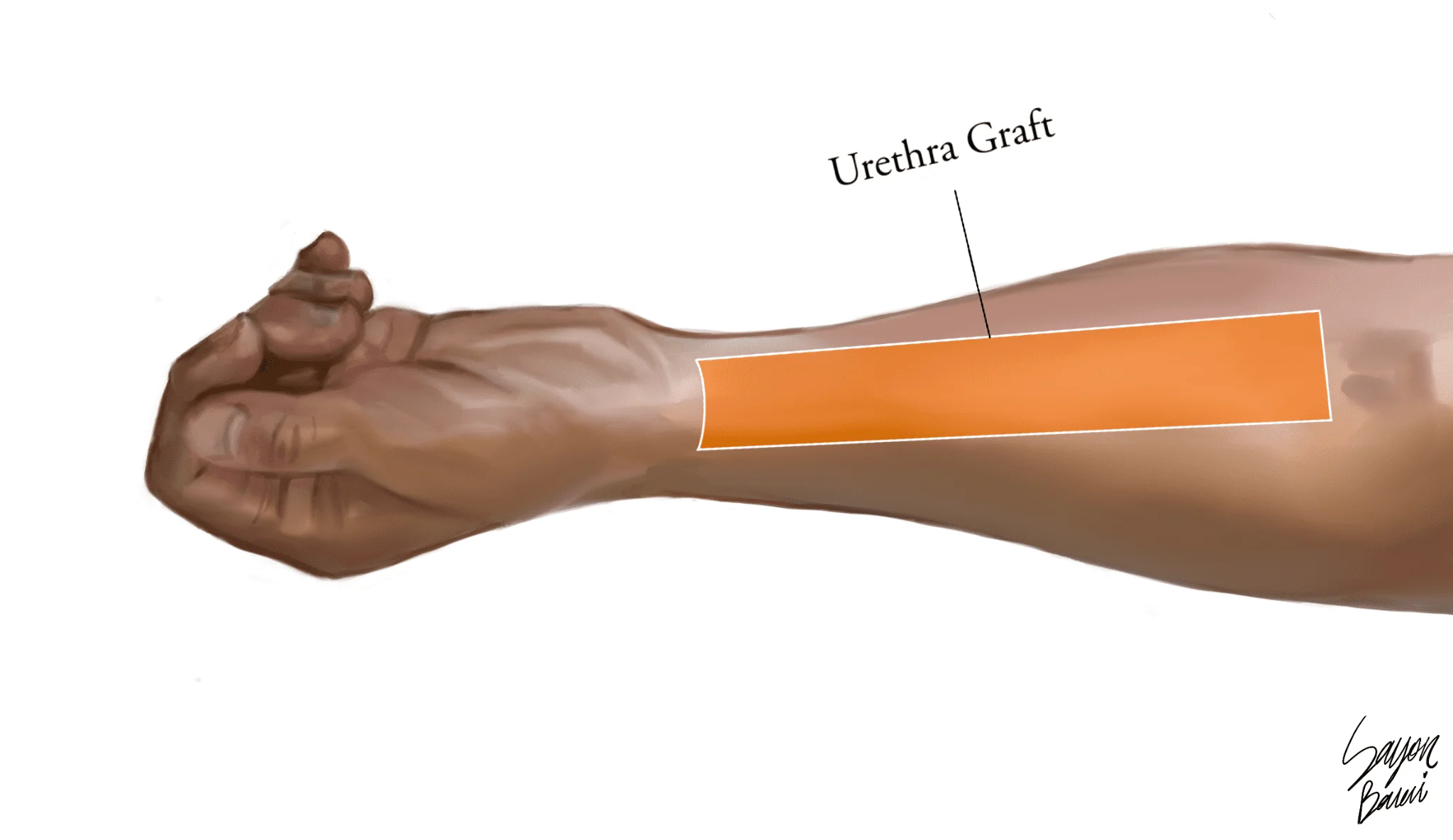
- Hair Removal Preparation: Patients that would like to undergo an RFF phalloplasty or have a urethral graft taken from the forearm must undergo hair removal to this area prior to surgery.
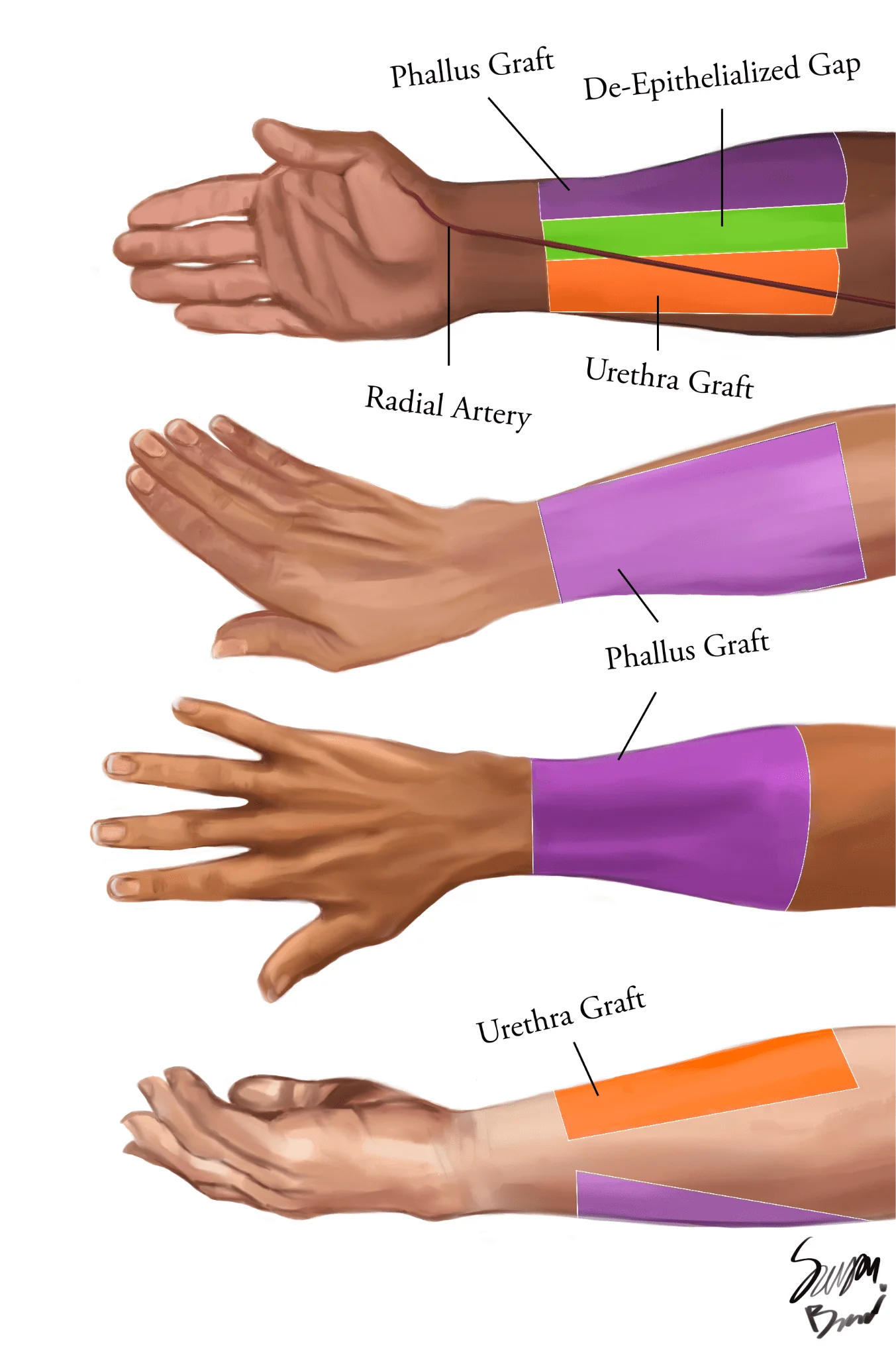
Please note that permanent hair removal is only required for the section of the forearm (highlighted in orange on the illustrations) that will be used as a graft to extend the urethra out to the tip of the penis. This is due to the fact that hair growth inside of the urethra can cause a variety of complications. For more information, click here
- BMI Requirements: Unlike other surgeries offered at the GCC, there are strict BMI requirements for many bottom surgery procedures due to the high risk of complications and surgical failure, especially in the case of phalloplasty. You can read about Dr. Ley’s BMI candidacy requirements here.
- Support letter: Bottom surgery patients, especially when seeking out insurance approval, often need to present one or more support letters from a licensed mental health professional. For more information on the requirements for the procedure you are interested in, you can request a consultation and our team can get back to you.
- Lifestyle Adjustments: Quit smoking for at least 4 weeks prior to surgery and make any necessary lifestyle changes to optimize your overall health and reduce complications during recovery. Please note that before undergoing microsurgery (e.g., nerve innervation for an RFF phallo), patients who have a smoking history may need to take a nicotine and cotinine exam, as any tobacco use can cause surgical failure.
- Support System: Regardless of whether or not you will be spending time in the hospital after surgery, bottom surgery recovery is known to be very physically and emotionally taxing. Having a strong support network of family, friends, support groups and/or a mental health professional is crucial. Organizations like Quest House in San Francisco offer bottom surgery patients a safe place to stay while they recover.
- Leave Planning: Consider your options for medical leave. Prior to your operation, your surgeon’s office will let you know how much time you will need to take off from work and provide you with the proper documentation to solicit leave.
- Financial Planning: Explore insurance coverage and plan for the costs associated with the surgery, potential follow-up procedures or revisions, and taking time off from work. Please note that the GCC only offers phalloplasty for patients with insurance coverage at this time due to hospital restrictions.
Recovery and Aftercare
The recovery process after masculinizing or “FTM” bottom surgery can be lengthy and challenging. You can find more specific recovery instructions for metoidioplasty here and phalloplasty here. It is important to be patient and allow your body the necessary time to heal and adjust to the physical changes of bottom surgery. Adhering to your surgeon’s instructions and seeking support when needed can help ensure a successful recovery and long-term satisfaction with your results.
- Initial Hospital Stay: Some procedures (i.e., simple metoidioplasty) can be performed as an outpatient procedure, meaning you will be released home the same day as your surgery. With most bottom surgery procedures, patients can expect to remain in the hospital for at least 1-2 days after surgery for close monitoring and initial recovery.
- Medications: Your surgeon will prescribe pain medication to help manage any pain and discomfort that are common in the initial weeks following surgery. Antibiotics may also be prescribed in order to prevent infections.
- Wound Care: Proper wound care, including application of ointments, dressing changes, and hygiene, is crucial to prevent infections and promote healing. You and your support person will receive detailed instructions after your surgery.
- Catheterization: Depending on the procedure performed, a catheter may be in place for days or weeks after to allow for proper urethral healing and function.
- Activity Restrictions: Strenuous activities, heavy lifting, and sexual activity will be restricted for several weeks or months to allow for adequate healing.
- Follow-up Appointments: Follow-up appointments with your surgeon are essential to monitor healing progress, address any complications, and discuss potential revisions or additional procedures.
- Psychological Support: Seeking counseling or support groups can help manage the emotional and psychological aspects of the recovery process. As patients navigate pain, discomfort, being bed-bound, activity restrictions, and more, they may experience temporary feelings of depression or even regret during recovery. Once patients heal, they express overwhelming amounts of joy and satisfaction.
Click Here to Request the Next Steps to Schedule a Consult!
We offer complimentary virtual and in-person consultations with our board-certified surgeons. Click here to complete our consultation request form to learn more about the next steps in your patient journey.
BOOK CONSULTATION
Suite 1010, 450 Sutter St
San Francisco, CA 94108
Phone: (415) 780-1515
Fax: (628) 867-6510
GCC business hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
Board Certification
& Memberships
Copyright © 2023 GCC (Gender Confirmation Center). All Rights Reserved.