

The Comprehensive Guide to Inverted T Top Surgery: Maintaining Sensation and Volume
Medically reviewed by Jennifer Richman on September 15, 2024.
Understanding the Inverted T Anchor Top Surgery
The inverted T or anchor incision for chest reconstruction or breast reduction, like the buttonhole incision, has the potential to preserve heightened nipple sensation. This is made possible because an inverted T top surgery does not remove all chest tissue, as is the case with the double insicion. Rather, the surgeon leaves behind what we call the pedicle: a portion of tissue that they estimate to contain enough of the original blood and nerve supply to keep the nipple and areola alive. You can read more about why patients choose this procedure, the results, scarring and recovery process below.
Patients interested in having more precise control over the shape and position of the areolas and nipples after surgery, a free nipple graft can be performed with the inverted T or most other procedures. Below we explore why chest reconstruction and breast reduction candidates might pursue an inverted T incision with or without a free nipple graft.
Is the Inverted T Anchor Top Surgery Right for Me?
The inverted T technique is often selected by transmasculine, non-binary and gender non-conformming individuals seeking a chest reconstruction or chest/breast reduction. The following is a list of common reasons why patients choose this incision for their gender-affirming top surgery:
- Nipple Sensation: Maintaining heightened levels of nipple sensitivity is a top priority for your top surgery results. By heightened sensitivity, we mean the heightened ability to detect pressure and temperature in the nipple-areola complex.
- Maintaining Chest Volume: You are not interested in achieving complete chest flatness. For instance, this procedure is often pursued by plus-sized, transmasculine patients who would like the volume of their chest to be proportional with the size of their abdomen and the amount of fat present in the rest of their body. Some non-binary patients describe the results of this procedure as giving them a more gender-fluid look: it allows them to easily conceal or reveal their chest tissue depending on their clothing.
- Aggressively Reducing Chest Volume: You are interested in having a drastic reduction in breast tissue volume similar to a traditional breast reduction. In other words, you are interested in maintaining a somewhat teardrop shape, having minimal breast overhang, and a bit of movement of the chest (i.e. “bounce”) after surgery. This option is frequently pursued by patients who want the flexibility of maintaining some tissue but experience dysphoria or discomfort with a larger chest.
- Pectoral Muscle Appearance: You are ok with pectoral muscle definition not being as visible. This is because the leftover pedicle tissue will slightly conceal the chest muscles below.
- Nipple Size and Placement: You are fine with not having complete control over the repositioning and resizing of your nipples. That said, areola resizing (i.e., making your areola smaller) can still be done with the hope of keeping the areola and nipple sensation completely alive like before.
If you are interested in achieving a complete level of flatness and having greater control over the size and position of your areolas through top surgery, you can read more below about how the inverted T incision compares to the double incision with a free nipple graft, as this might be a more suitable option for you. That said, patients who would like to obtain a flat chest without sacrificing heightened nipple sensitivity can undergo a nerve reconstruction double incision procedure.
Preparation and Candidacy for Top Surgery
Preparing for inverted T top surgery involves several important steps:
- Consultation: The first step to initiating your top surgery journey is scheduling a consultation with a board-certified surgeon. At the GCC, all of our consultations––whether virtual or in-person––are free of charge to patients. This is an opportunity to discuss your medical history, goals for surgery and get any specific questions you have answered by a surgeon.
- General Requirements for Top Surgery: The GCC is one of the few gender-affirming surgical practices in the US that does not require that patients meet certain Body Mass Index (BMI) requirements nor that they undergo hormone replacement therapy (HRT) to be candidates for top surgery. However, patients must stop smoking and quit nicotine altogether at least three weeks before surgery. Likewise, patients cannot consume alcohol the week before and after top surgery.
- Candidacy for Inverted T Top Surgery: Generally speaking, this technique works on patients of varying types of skin elasticity. The inverted T or anchor incision allows for the surgeon to remove any overhang of skin that the patient would like to have excised. This technique works best for patients who have a medium to large amount of tissue starting out. The buttonhole procedure gives patients similar results in terms of volume and sensation, but is meant for those who have less tissue starting out.
- Medication and Supplement Adjustments: Certain medications, supplements, and herbal remedies may need to be discontinued temporarily to minimize anesthesia complications, bleeding risks and optimize healing. Please let your surgeon know in your consultation which medications and supplements you are currently taking.
- Arrange for Support: Plan for post-operative care and assistance, as you may require help with daily activities during the initial recovery period. During your first three weeks post-op, you will not be able to lift more than 5 lbs nor will you be able to lift your arms above your shoulders. For this reason, we recommend that you have support people help you with everyday tasks.
Procedure Details
The inverted T top surgery typically follows these general steps:
- Anesthesia: The procedure is performed under general anesthesia to ensure your comfort and safety.
- Incisions: The surgeon will make incisions around the areola and a vertical incision extending downward from the areola, forming an inverted “T” shape.
- Tissue Removal and Sculpting: Excess breast tissue and skin are carefully removed, and the remaining tissue is sculpted to create the desired chest contour.
- Nipple Repositioning: The nipple and areola complex is repositioned to a more masculine location on the chest. The nipple and areola complex stays attached to the pedicle during an inverted T top surgery without nipple grafts, so repositioning will be somewhat limited by the tethering of the tissue to the pedicle.
- Closure: The incisions are meticulously closed with sutures or surgical adhesives, and dressings are applied to protect the surgical site.
It’s important to note that the specific technique may vary depending on the surgeon’s experience and the individual patient’s anatomy and goals.
Recovery and Aftercare
The recovery period after inverted T top surgery can vary, but generally, you can expect the following:
- Immediate Postoperative Care: You may experience some discomfort, swelling, and bruising initially. Your surgeon will provide pain medication and instructions for caring for the surgical site.
- Drainage Tubes: Temporary drainage tubes may be inserted to prevent fluid accumulation and promote healing. Drains are placed in the chest after top surgery to prevent any fluid buildup (i.e. seroma) when liposuction is conducted and/or larger amounts of tissues are removed.
- Activity Restrictions: Patients should not lift more than 5lbs nor lift their arms above shoulder height for the first three weeks after surgery to allow proper healing. Likewise, patients will not be able to shower or bathe until their dressings and/or drains are removed at the first post-op appointment (about 6-8 days after surgery). In the meantime, patients can take sponge baths or wet towelettes, being careful not to wet the surgical site.
- Scar Management: Your care team will provide guidance on incision care and scar management techniques, such as massage and silicone-based topical treatments, to minimize the appearance of scars, usually starting around 3 weeks post-op.
- Follow-up Appointments: Regular follow-up appointments with your surgeon are essential for monitoring your healing progress and addressing any concerns or complications. Patients that come in from out of town will need to stay until the first post-op appointment (about 6-8 days after surgery) to have their dressings removed and healing monitored.
Frequently Asked Questions (FAQ)
-
 How long does inverted T top surgery take?
How long does inverted T top surgery take? -
The duration of the inverted T top surgery procedure can vary depending on the individual’s anatomy and the extent of tissue removal required. On average, the surgery typically takes 2 to 4 hours.
-
Will I lose nipple sensation after inverted T top surgery?
-
While some loss of nipple sensation is common after any top surgery procedure, the inverted T technique is designed to preserve as much nipple sensation as possible. Many individuals report retaining some degree of nipple sensation, although the level of sensation can vary.
-
Can I have inverted T top surgery if I have large breasts?
-
Yes, the inverted T technique is generally recommended for individuals with a medium to large amount of tissue they would like to be removed.
-
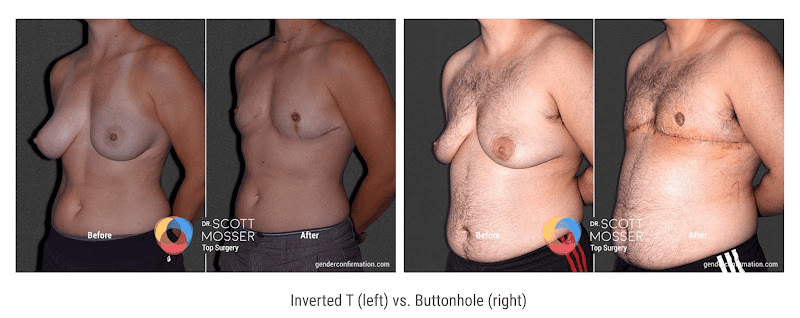
Which procedure is right for me: the inverted T vs. the buttonhole incision?
-
The deciding factors to help a patient choose between these two procedures are (1) the amount of excess skin that needs to be removed and (2) the patient’s desired aesthetic goals. First, the inverted-T, as opposed to the buttonhole, is recommended in patients with greater amounts of breast tissue and/or excess skin to remove. The vertical incision made between the areola and the lower, horizontal incision is what allows for excess skin removal and is the only factor that differentiates this procedure from a buttonhole. Second, the inverted-T tends to result in more teardrop shaped results, whereas the buttonhole procedure leaves a more moundlike shape.
-
Which procedure is right for me: the inverted T vs. the double incision?
-
Using the inverted-T method means the nipple and areola do not need to be placed as a free nipple graft, as it does with double incision. As a result, inverted-T may result in a better chance of maintaining pre-surgery levels of nipple sensation, though this outcome is not certain. As a tradeoff, the double incision is ideal for patients who want flatter results. That said, patients that are interested in a flat chest while maintaining heightened nipple sensation may be good candidates for the double incision with nerve reconstruction.
Another factor to consider if deciding between these two procedures is the location of postoperative scars. The double incision sometimes leaves the possibility of scars that are less visible or more tucked away. The inverted-T leaves an extra, more visible, vertical scar between the areola and the inferior incision. Additionally, with regards to scar placement, the lower curvature of the incision is not as customizable by the surgeon because it has to be located in the lower chest fold. In other words, the surgeon cannot customize the horizontal incision as much as they could with the double incision approach.
Request a Free Surgical Consultation Today.
All virtual and in-person consultations with our board-certified surgeons are free. Once you fill out this form, our patient care team will reach out and guide you through every step to get to surgery.
Suite 1010, 450 Sutter St
San Francisco, CA 94108
Phone: (415) 780-1515
Fax: (628) 867-6510
GCC business hours are from 9:00 am to 5:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
Board Certification
& Memberships

![]()
![]()
Copyright © 2023 GCC (Gender Confirmation Center). All Rights Reserved.